Here I am, still fighting the ebb and flow of this recent recurrence of the stuck music (auditory memory loops/AMLs). (I now suspect I have gotten a bad box of estrogen patches, and will see if this resolves when I start on the new box.) Meanwhile, I decided to try searching OCD (obsessive compulsive disorder) sites for new perspectives.
Do I really have OCD?
The first thing I looked at was a self test for OCD. I failed miserably (or should I say “happily”). Classic OCD is associated with repetitive rituals (like locking the door the “right” number of times, or incessant hand washing) and a lot of dark thoughts and fears. The TV character Adrian Monk had OCD (among other issues). His list of fears/phobias began with “Germs, needles, milk, death….” Yes, in that order.
I apparently don’t have OCD in the sense these tests define it. I have no rituals, no dark thoughts, and no phobias/fears other than: (a) spiders (since childhood), (b) 4-leaf clovers (long story), and, most important, (c) the fear of having songs stuck in my head again and not being able to enjoy…or even truly live life.
OCD – Melanie’s Article
Despite my apparent lack of OCD symptoms, I searched for OCD and hormones and came up with a fabulous article from Melanie Gladney’s HubPage. http://melaniegladney.hubpages.com/hub/OCD-Glucose-Metabolism-and-Food-Allergies This focuses on classical OCD, but offers suggestions that may work for some of us as well. It is certainly worth a shot.
OCD and Hormones
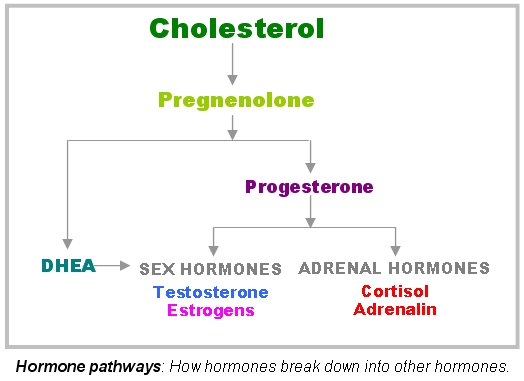
In this article, she discusses the same hormonal influences I’ve identified, but she adds important dimensions to the discussion, including information about key brain chemicals that the sex hormones trigger.
She emphasizes the role of progesterone in calming anxieties. Just keep in mind that, for me at least, there is a very narrow sweet spot for progesterone levels: if I get too much (relative to estrogen), it actually brings on the stuck music. But as we know, we all have different body chemistries and reactions, so keep progesterone in your toolbox and use it carefully, like everything else.
OCD and Blood Sugar, Insulin Resistance and Cortisol
More important, Melanie covers in great detail the role of blood sugar/metabolism and food allergies as they may relate to OCD. Her suggestions about diet require more self discipline than I am easily capable of, but they have worked for her OCD, so please check them out and see if her suggestions might work for you.
Remember that high cortisol can not only trigger or exacerbate the AMLs, it can induce insulin resistance (which Melanie talks about in easy-to-understand detail). So maybe it’s not the cortisol directly that affects our AMLs after all, but the insulin/metabolic conditions that result from that cortisol overload. Maybe regulating blood sugar and/or insulin is, in fact, the answer…or at least part of it.
Is it that simple? Probably not.
From a logical standpoint, it seems that if blood sugar, food allergies, and insulin resistance were truly at the root of this (in my case, at least), then I should not have been able to get rid of the AMLs when I implemented my current hormone regimen, because I did not change my diet. The only things I changed were: (1) I took cortisol suppressing supplements, and (2) I created a mini hormone cycle with a surge of estrogen 24 hours before I took my progesterone.
This same kind of reasoning told me that it’s not just cortisol that triggers the AMLs, because I have been way more stressed in my younger life (i.e., had tons of adrenalin and cortisol surging through my body) and yet I did not get songs stuck in my head. This only started when my sex hormones went south at menopause…and it only went away again when I mimicked a youthful hormone cycle.
Then again, the most obvious difference between the identical twin boys who shared most everything except the AMLs was that the one who had the AMLs turned out to have a then-undiagnosed metabolic disorder involving insulin resistance. The mom obtained the diagnosis after reading about the cortisol/metabolic connection to AMLs here and taking her son in for relevant tests. So, clearly the AMLs and metabolic dysfunction are closely linked.
Visit Melanie
The bottom line is that Melanie and I seem to be running down the same rabbit hole, chasing the same two suspects–sex hormone imbalances and dysfunctional metabolic/adrenal processes–from slightly different perspectives. So I encourage you to check out her hub. (You can read the articles but may have to join HubPages.com to comment.) And write to her if you think she can help. She seems to be very generous in responding.
And if any of you try her suggestions, please keep us posted on the results, whether positive, negative or neutral.
Wishing you a blissfully quiet day.
Pat
BTW, Last night I attended a lecture by a neuroscientist, and he has promised to put me in touch with someone he thinks might be able to help us or at least can point us to someone else who might. Cross your fingers…